Brian holds a Master degree in Health Administration (MHA), a Bachelor of Science in Health Sciences (BSHS), and a Certificate in Clinical Bioethics which bestows the ability to serve on ethics boards, help make healthcare decisions, and provide continuing medical education.
He is a national author and speaker and health consultant in all aspects of healthcare delivery, with special interests in risk adjustment, population health, public health, clinical bioethics, patient safety, and patient education.
*All posts and materials posted here are for education and demonstration purposes and are not intended to be medical advice. It is important to remember that every person is unique with unique diagnoses, and may be taking different prescriptions and supplements. I encourage each person to discuss your conditions with a trusted healthcare provider and be engaged to learn along your individual path to wellness.
If we are honest about our current state, while we have made great strides in new discoveries and treatments for a great number of conditions, our system has never been more fragile.
The general public is increasingly distrustful of healthcare providers and the “system.” Part of this is directly related to the very poor handling of communication of the COVID pandemic. Other parts affecting this view include the many months-long wait for an appointment that many experience across the USA, the moral injury of not only providers like doctors and mid levels (NP’s and PA’s), but also that of nurses that has led to a shorter temperament and sometimes a less than ideal caring environment. We had a shortage of providers before the Affordable Care Act (ACA) was passed, and after its passing there was an even larger deficit. Then not long afterward, we were met with a worldwide pandemic like we have never seen and lost many providers to both illness and resignation over frustrations of seeing patients die.
Those providers who have stayed the course, or joined in the effort of delivery of care are trying to steady the helm, but there is an ongoing stress related to long lines to be seen, lack of time to talk with patients or provide quality patient education, and patients who aren’t sure whom they can trust in many situations. It is a very scary feeling to be extremely ill and afraid if your provider is taking your symptoms seriously or if it feels they don’t have time for you. I hear this over and over again and have personally experienced this myself, and witnessed it with my own family members across many facilities and providers, and I have over 35 years of experience in healthcare.
While we are tending to patients to heal the sick, we are now tasked with simultaneously healing the system, and this task cannot be taken lightly. It will take some time to rebuild trust, and to equalize the number of providers that are needed for the populations across the country.
Hopefully, with more patient education, we can assist by helping people to help themselves through a better understanding of their various ailments and measures they can take themselves at home before running to the doctor for everything. This will then hopefully free up some of those coveted appointments for those who are in more immediate need and help to lessen some of the extreme stress placed on our healthcare system as a whole.
This health blog is designed with an idea of empowering people with trusted information about healthcare issues so that they may be able to not only better understand the healthcare system and challenges, but also how we can live healthier lives and try to avoid and/or reverse chronic illnesses where possible. Many believe that patients lack any self control or governance in how they live and eat, and this leads to an immediate move to prescribe something for every single issue, but I believe in the power of people to evolve, and learn, and to place more effort on living in a more healthful manner. It will not be easy as many company’s place addictive substances in their products because they want you to buy more, but strengthening willpower to become more independent and focusing on wellness will help in some way for every person, so do what you can to help yourself. This self help to wellness is the ultimate exercise of self love.
Brian holds a Master degree in Health Administration (MHA), a Bachelor of Science in Health Sciences (BSHS), and a Certificate in Clinical Bioethics which bestows the ability to serve on ethics boards, help make healthcare decisions, and provide continuing medical education.
He is a national author and speaker and health consultant in all aspects of healthcare delivery, with special interests in risk adjustment, population health, public health, clinical bioethics, patient safety, and patient education.
*All posts and materials posted here are for education and demonstration purposes and are not intended to be medical advice. It is important to remember that every person is unique with unique diagnoses, and may be taking different prescriptions and supplements. I encourage each person to discuss your conditions with a trusted healthcare provider and be engaged to learn along your individual path to wellness.
While our world has grown in technological and scientific accomplishments, many have become consumed with newly evolved living habits that may not offer the healthiest of choices. It sometimes seems that with our fast paced living, thoughts of wellness have been sidelined while we are constantly fed promises of pills and other pharmaceutical treatments that are often unnecessary if we adjusted our way of living.
Every living thing needs clean air, clean water, and clean food for consumption, yet we have many failing water systems, pollution filling our air, and foods that are not only fast, but also pumped full of chemicals and hormones that can be harmful to life itself. Shockingly, some of the very institutions that were formed to protect the public, allow for certain levels of chemicals and additives that are known to be harmful. The problem here is that no one can accurately estimate the volume of these substances that are consumed by each individual over time. Over time, these unnatural additives can contribute to, and/or cause disease or illnesses and sometimes hasten medical problems and even shorten the lifespan of people.
It is estimated that 80% of known chronic conditions can be avoided with diet and lifestyle modifications, thereby reducing the need for medical intervention. There are of course some conditions like genetic disorders and life accidents that cannot be avoided. Yet, there are a great number of opportunities to improve many chronic conditions through healthy living choices and diet modifications.
We are constantly advertised to for this drug or that one (always with the quick rundown of potential side effects, often including death) but every medication comes with strings attached. Many without medical knowledge have a false impression that medicine can cure almost anything. It cannot. There are many limitations to what can be fixed or remedied. In an ideal world, everyone should be able to focus on healthier living to avoid the need of medical intervention wherever possible. Finances and family schedules can interfere with this goal, but if we collectively concentrate on changing our living environment standards, to include our standards for clean healthy foods, then over time, we can change how we live and improve our quality of life with less disease and illness.
There are also many dietary choices, herbal remedies, and other supplements that can help the body to correct off balanced items and change the course of some chronic conditions, but its always important to discuss these things with your trusted healthcare provider. There are sometimes side effects, and some of these interventions can affect or interact with other medications.
It is absolutely unfair and incorrect that healthier options always cost more and the detrimental junk foods are cheaper. While the economy and personal finances certainly affect the choices that people make, if enough people become more educated and concerned for the utmost of health possibilities, then pressure from the marketplace can influence not only the products being offered in becoming more health conscious, but also help stabilize the prices of those items.
One of the goals of this blog is to educate on healthcare matters and providing new ideas to promote lifestyle changes is one of those goals. Within each chronic condition, we will attempt to provide tools and educational information specific to that condition, diagnosis or illness, that can assist you on your wellness journey.
You can use the search bar on this blog to look up various conditions and we will be updating information regularly on current topics as well as adding new ones for your consideration. All information is carefully crafted with the intent to provide accurate and ethical principles in a manner that can be easily understood, while also reliable as truthful because trust is a number one priority in healthcare. As always, we truly wish you well.
Brian holds a Master degree in Health Administration (MHA), a Bachelor of Science in Health Sciences (BSHS), and a Certificate in Clinical Bioethics which bestows the ability to serve on ethics boards, help make healthcare decisions, and provide continuing medical education.
He is a national author and speaker and health consultant in all aspects of healthcare delivery, with special interests in risk adjustment, population health, public health, clinical bioethics, patient safety, and patient education.
*All posts and materials posted here are for education and demonstration purposes and are not intended to be medical advice. It is important to remember that every person is unique with unique diagnoses, and may be taking different prescriptions and supplements. I encourage each person to discuss your conditions with a trusted healthcare provider and be engaged to learn along your individual path to wellness.
The heart is a uniquely special and important organ. Medical issues that can occur with the heart can involve many areas to include blockages of the vessels, issues with the fitness of the muscular tissues of the heart, infections of the heart, valve issues, and various rhythm issues which are commonly known as cardiac conduction disorders. These rhythm issues are presented below.
Cardiac Conduction Disorders
Common cardiac conduction disorders include supraventricular tachycardia, AV blocks, sick sinus syndrome, atrial/ventricular fibrillation, and atrial/ventricular flutter.
It is helpful to have a basic understanding of how the heart’s electrical system works before discussing the various conduction disorders that can occur. The heart is a muscle, which also has its own electrical system. Many may be more familiar with cardiac problems that can occur due to arterial clogging or blockages, such as coronary artery disease (CAD), or there may be a disease complication affecting the muscle of the heart causing it to become weak, such as in cardiomyopathy. When the electrical impulses have problems or difficulties, a cardiac conduction disorder may occur. There are many different types of cardiac conduction disorders and some patients can experience these intermittently, while others may persist for a chronic period of time or may be life-long. Some patients have more than one conduction disorder simultaneously. Possible treatments for conduction disorders include surgery, ongoing medication and observation, or an electrical assistive device implant.
The Sino Atrial (SA) node, located in the upper right quadrant of the heart, is the pacemaker of the heart. The SA node sends an electric signal that prompts the heart to contract/pump. When this signal is blocked, interrupted, sent too frequently or infrequently, or the ventricular response is out of sync, conduction disorders may occur. Conduction disorders can develop over time, can be caused by medications, consuming other supplements, foods, or drinks, or can be congenital.
Think of the heart as a square with upper and lower portions. Example:
Chambers of Heart Example
Right Atrium
Left Atrium
Right Ventricle
Left Ventricle
Simplistic view of heat chamber positioning
Measure of Heart Rate Example
Source: Google Images, Web 2024
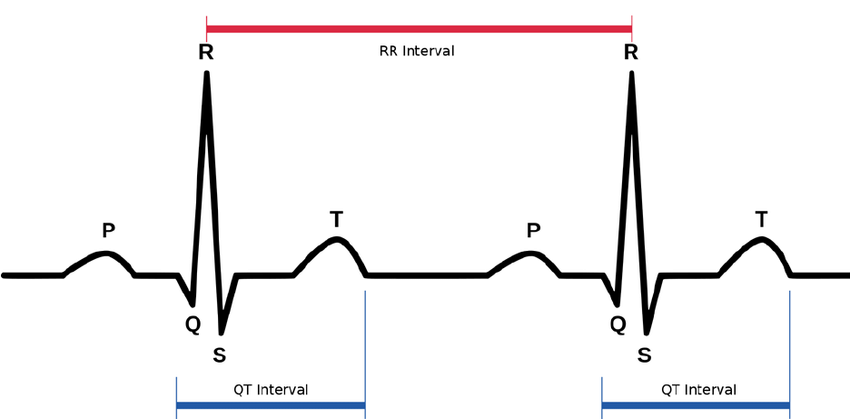
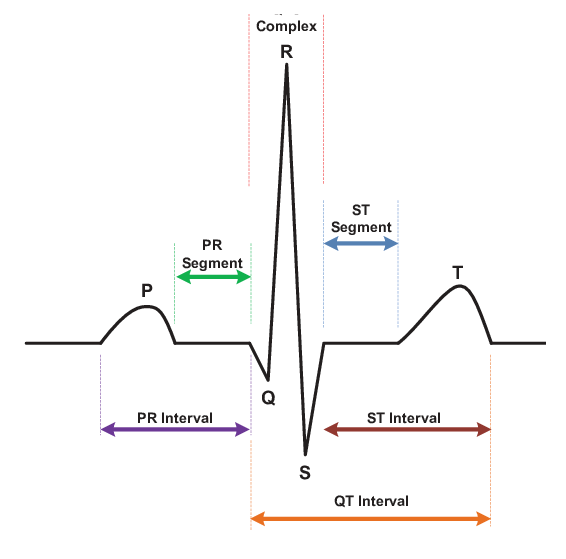
In the diagram above of a normal heartbeat, the “P” is the SA node’s (Right Atrium) electrical impulse for the heart to pump or beat, the QRS is the ventricular (Right & Left Ventricles) response (heartbeat), and the “T” is a re-polarization of electrical energy for the process to repeat itself. These points are measured when reviewing various heart conduction disorders and help identify where the conduction disorders may be occurring.
Various intervals between complexes are measured to analyze heart rhythms.
Figure: Heartbeat Dissected
Source: Google Images, Web 2024
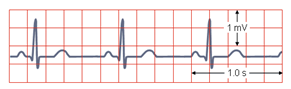
In a NSR (Normal Sinus Rhythm), all complexes are normal, evenly spaced, with a rate of 60-100 beats per minute.
Example of Normal Sinus Rhythm
Source: Google Images, Web 2024
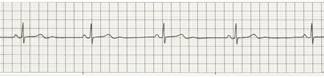
Bradycardia is a slower than normal heart rate. Tachycardia is a faster than normal heart rate. Both are a normal part of daily heart function and response.
Example of a Sinus (normal) Bradycardia
Source: Google Images, Web 2024
Example of a Sinus (normal) Tachycardia
Source: Google Images, Web 2024
An extremely slow or persistently-below-normal heart rate often is due to a malfunctioning SA node. The condition is called sick sinus syndrome. The typical intervention for a sick sinus syndrome is the placement of a pacemaker to make the heart rate normal again. Various pacemaker models may be used.
Everyone’s heart rhythms vary, based on physical and emotional status, nutrition, and temperature. Each person’s pulse, or heart rate, can change from minute to minute. Likewise, heart rate will speed up (tachycardia) or slow down (bradycardia) as a response to physical and emotional factors. Cardiac conduction disorders can occur when these heart rates go too far beyond normal parameters (whether too fast or too slow). Many people will have skipped beats and bouts of fast and slow heart rates as a part of everyday life experiences. Only when these conduction disorders persist, create symptoms that would cause a concern for compounded problems, or are not addressed do they become a problem.
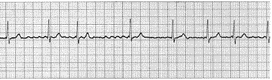
When a faster than normal heart rate originates at or above the atrioventricular node (AV), the condition is supraventricular tachycardia (SVT). Atrial fibrillation is a type of supra ventricular arrhythmia. In A-Fib (atrial fibrillation), there are irregular impulses reaching the AV node and only some are being transmitted. Another type of SVT is documented as paroxysmal supraventricular tachycardia (PSVT). The word paroxysmal means that there is a sudden burst or display of the tachycardia in portions or waves where there is a great intensity, which calms and then bursts forth in display again. A supraventricular tachycardia is a rapid atrial rhythm, while a ventricular tachycardia is a rapid ventricular rhythm.
Example of a Supraventricular Tachycardia (SVT)
Source: Google Images, Web 2024
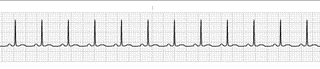
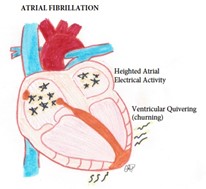
Atrial Fibrillation/Flutter
Atrial Fibrillation
Source: HAA
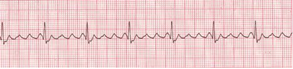
Example of Atrial Fibrillation
Source: Google Images, Web 2024
In the above examples, a clear difference between a normal heart rhythm and atrial fibrillation is clearly demonstrated. The placement of the P, QRS, and T waves are obviously out of rhythm. This is from the intense “shaking” or “churning” of the ventricles from the atrial hyperactivity or rapid firing of impulses. Atrial fibrillation is a very common diagnosis that is usually managed through blood thinning medications (such as Coumadin or warfarin) to prevent clots from forming from the churning activity. Sometimes atrial fibrillation can be a short event or converted and other times it is a life-long diagnosis. In some cases, a pacemaker may be implanted for the treatment of A-Fib, and if the patient has more than one conduction disorder, for example a history of sick sinus syndrome (or SA node malfunction) as well as A-Fib, and there is a pacemaker in place, the patient likely still has A-Fib and this can be revealed by the current use of Coumadin or warfarin, other blood thinner, or A-Fib medication. Pacemakers are most often implanted for SA node malfunction or sick sinus syndrome and not for A-Fib.
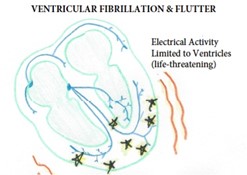
Ventricular fibrillation is a condition in which there is uncoordinated contraction of the cardiac muscle of the ventricles in the heart, making them “quiver” rather than contract properly. It is life threatening and requires immediate attention for life-saving purposes. Ventricular flutter is an arrhythmia, more specifically a tachycardia that affects the ventricles with a rate of over 200 beats per minute. It has been considered as a transition between ventricular tachycardia and fibrillation. It is a critically unstable arrhythmia that can result in sudden cardiac death. Both of these conduction disorders require cardioversion (shock treatment) as well as medication support. Patients who have had known problems with short runs of these arrhythmia’s may be placed on an Automatic Internal Cardiac Defibrillator (AICD) which is a special pacemaker than can monitor for problem rhythms and shock the patient when necessary.
Ventricular Fibrillation/Flutter
Source: HAA
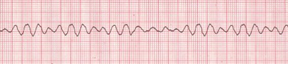
Example of Ventricular Fibrillation
Source: Google Images, Web 2024
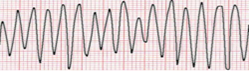
Example of Ventricular Flutter
Source: Google Images, Web 2024
Atrioventricular (AV) Block
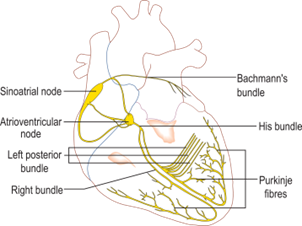
When the SA node sends its electrical impulse downward through the heart, the electrical impulse runs along a normal pathway. These bundles (or electrical lines) can become blocked for various reasons, causing a “bundle branch block.” When this occurs, something is blocking the normal flow of the signal, which results in a form of AV block. There is a disruption of the electrical message between the atrium (top of the heart) and the ventricles (bottom of the heart).
Documentation of AV blocks is important because there are many different types of blocks. The blocks are classified by measurements of the PR interval in the heartbeats (mentioned earlier) and are often named for physicians who discovered them.
Electrical System of Heart
Source: Google Images, Web 2024
First Degree AV Block: PR interval is greater than 0.20 sec.
Second Degree AV Block:
Type I (also known as: Mobitz I, or Wenkebach): Progressive prolongation of PR interval with dropped beats (the PR interval gets longer and longer, and finally one beat drops).
Type II (also known as: Mobitz II, or Hay): PR interval remains unchanged prior to the P wave, which suddenly fails to conduct to the ventricles.
Third Degree AV Block (Complete): No association between P waves and QRS complexes.
Bundle Branch Block: General defects in the electrical conduction system of the heart between the atrial and ventricle portions of the heart. Bundle branch blocks are fairly common and often do not cause any issues.
Heart conduction disorders can be serious. some patients might discount dizziness or fatigue to the causes of their symptoms, and older patients may experience age prejudice related to potential dementia or simple aging when a cardiac condition may be underlying. It is important to discuss all symptoms in detail with your healthcare provider so that the appropriate tests can be performed.
Diagnostic testing can include blood work, cardiac monitoring, exercise stress testing, and echocardiograms. Such testing is chosen based on the symptoms being presented in an effort to discover what issues might be present and which treatments might be best for each patient.
Brian holds a Master degree in Health Administration (MHA), a Bachelor of Science in Health Sciences (BSHS), and a Certificate in Clinical Bioethics which bestows the ability to serve on ethics boards, help make healthcare decisions, and provide continuing medical education.
He is a national author and speaker and health consultant in all aspects of healthcare delivery, with special interests in risk adjustment, population health, public health, clinical bioethics, patient safety, and patient education.
*All posts and materials posted here are for education and demonstration purposes and are not intended to be medical advice. It is important to remember that every person is unique with unique diagnoses, and may be taking different prescriptions and supplements. I encourage each person to discuss your conditions with a trusted healthcare provider and be engaged to learn along your individual path to wellness.
We are all living in unprecedented and unpredictable times. While there has been a lot of coverage on the importance of wearing masks when indoors or enclosed spaces, many have continued to challenge this health directive and many have compared this virus to the flu. It’s understandable because media coverage has continued to weigh these comparisons as well as others in leadership when discussing protocols, guessing possible outcomes, and more. My nearly 30 years of experience in healthcare in both clinical and leadership positions has taught me that when you want to convey information, there are important considerations if you really want to see understanding and behavioral change. Anyone who has tried to stick to a diet or stop smoking can confirm that it helps to become educated on what you are trying to achieve and I believe the most important part of education is the “why.” I’m told that as a toddler “why” was my favorite response to every new piece of information I heard and while I don’t recall that about myself, it only seems reasonable to want to know why something is, or why something should be, or why a recommendation has been made. I find patients are more compliant when they understand why. I hope to share enough here to help others understand how COVID-19 is different and why it’s dangerous to compare it to something as simple as the influenza (flu) virus. This is your why…
What Are Viruses?
A virus is a microscopic infectious particle that consists of an RNA or DNA genome enclosed in a protein shell. It is not able to reproduce on its own. It can only make more viruses by entering a cell and taking it over.
When a virus infects a host cell, it removes its protein coat and directs the host cell to transcribe and translate its genetic material. The hijacked cell assembles the replicated components into thousands of viral offspring, which can rupture and kill the host cell. The new viruses then go on to infect more host cells.
Viruses are usually classified by their morphology, their nucleic acid type (DNA/ RNA), method of replication, host organisms, and by the type of illnesses they cause.
DNA carries the genetic blueprint and instructions needed to create proteins, specific molecules essential to the development and functioning of the body. In viruses, RNA sometimes does this job.
DNA is double-stranded, while RNA is single-stranded. RNA contains ribose as a sugar, while DNA contains deoxyribose. Also, three of the nitrogenous bases are the same in the two types (adenine, cytosine, and guanine), but DNA contains thymine while RNA contains uracil.
General types of viruses (as experienced by humans):
1. Respiratory Viral Diseases:
Transmission: Contagious & spread by droplets in coughing or sneezing or contaminated objects like doorknobs, tabletops, etc. Essentially, they are spread mostly either from breathing in droplets in the nearby air or hands can become infected from touching infected objects where hand to face contamination can occur, and affect upper or lower parts of respiratory tract.
Duration: Historically most of these are what we would consider short lived. Most healthy people for example usually get over a cold in 7 to 10 days, flu symptoms are usually gone after about 5 days, and all symptoms are usually gone within 1 to 2 weeks.
Examples: Influenza (flu), Common cold, Some Adenoviruses, RSV (Respiratory Syncytial Virus), SARS (Severe Acute Respiratory Syndrome)
2. Gastrointestinal Viral Diseases:
Transmission: Contagious & shed in stool via bowel movements and can be spread in food or water contaminated by feces and sharing utensils or personal objects.
Duration: Most healthy people usually get over GI symptoms within a few days.
Examples: Norovirus, Rotavirus, Astrovirus, and Some Adenoviruses
Transmission: Contagious & spread by droplets in coughing or sneezing; Some like chickenpox and smallpox are spread through contact with fluid from broken skin lesions, while shingles can only develop in those who have had chickenpox when the varicella-zoster that was lying dormant awakens.
Duration: Most symptoms are usually gone within 1 to 2 weeks, although some like smallpox have stages that can last longer, but luckily, we have vaccines for these.
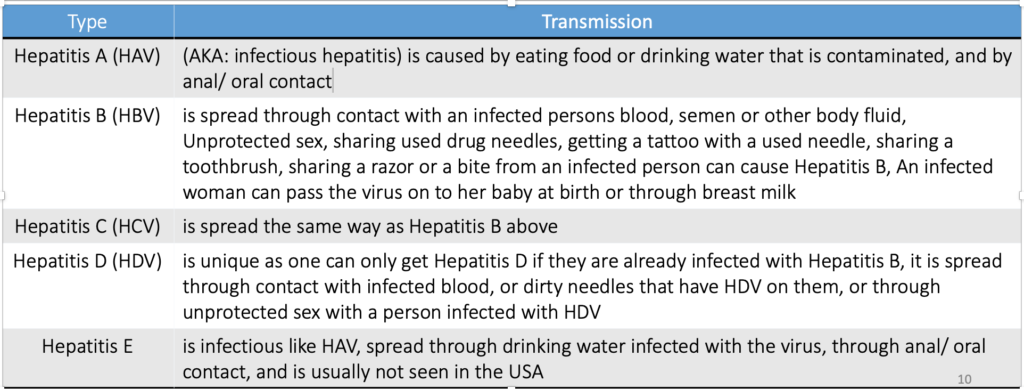
Transmission: Contagious & spread differently depending on type (see below examples)
Duration: Hepatitis A and E are typically short lived but the others are more serious and while we have a vaccine for Hepatitis B and some newer drugs for Hepatitis C that seem to eradicate the virus so far, Hepatitis viruses are still very serious and can be life-threatening.
Examples: Hepatitis A, Hepatitis B, Hepatitis C, Hepatitis D, etc.
5. Cutaneous Viral Diseases:
Transmission: Contagious & spread in various ways depending on type, they cause lesions or papules on the skin that can linger or disappear and reappear.
Duration: While there is no cure for most of these, and they are very contagious, they aren’t life-threatening.
Transmission: Contagious & spread differently by type. They are severe, deadly conditions that cause damage to the circulatory system. Dengue fever and yellow fever are spread through insect bites, Ebola is spread through contact with blood or body fluid, Lassa fever is spread by inhaling or consuming dried feces or urine from a rodent with the virus. There are no treatments other than trials and supportive measures
Transmission: Contagious & many are spread through the bite of an infected animal or bug (mosquitos and ticks). Poliovirus and other enteroviruses are very contagious and are spread through close contact with an infected person or contaminated objects.
Duration: Some of these can get better with treatment, but some are life threatening requiring hospitalization, and others can impair you for life.
COVID-19 is a novel (new) virus we have never seen before. This virus is different from other viruses, including other coronaviruses that we know about.
Virus name: SARS-CoV-2 Disease name: COVID-19
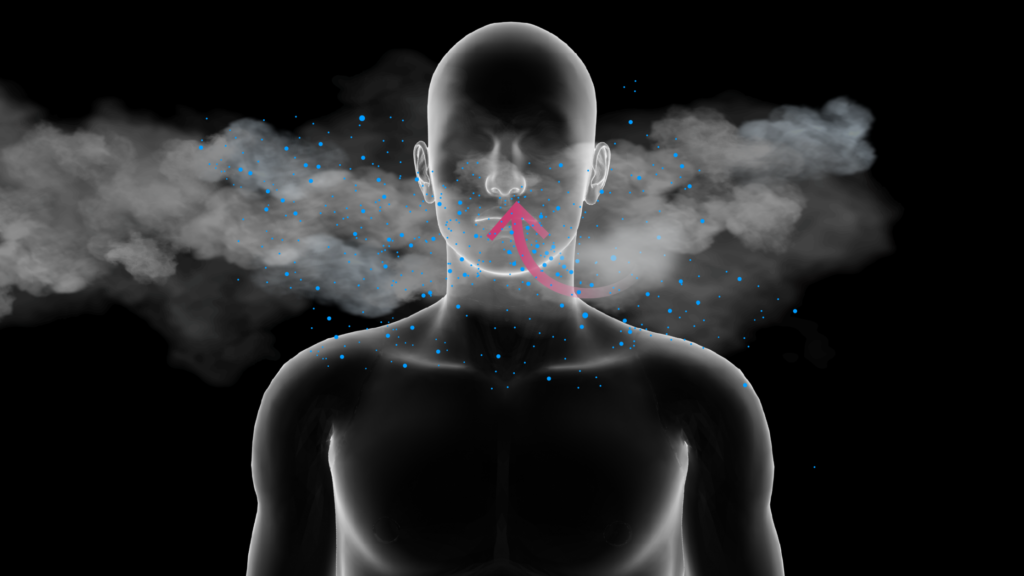
Symptoms may not appear for up to 2 weeks, and some may not show symptoms at all and be carriers. How the virus affects each person can vary based on factors like age, other medical problems that a person may already have, and how much of a “dose” of the virus the person took in when when infected.
Microscopic droplets in the air that you cannot see with the human eye are the reason masks are important.
Wearing Masks
What we know so far about COVID-19 is that it is spread mainly through 2 ways:
Person to person through droplets produced from an infected person when they speak, cough, or sneeze, and
Object to person (Fomite transmission) from objects touched like door knobs, utensils, coffee pot handles, microwaves, etc.) where an object is touched, and the hands are infected and then the infected hands touch your face or someone else’s before proper handwashing technique.
Mask wearing is not about personal liberties or choices. Allow me to explain: Someone I know is a breast cancer survivor and her office pressured everyone to come back into the office too soon. The leadership in that office had only instilled policies that you had to wear a mask coming into the building and that you could choose to remove your mask once you arrive to your cubicle or desk area and while they were asking people regularly about their potential exposures and taking temperatures they did not stop to consider fomite transmission from common objects within the office and they also did not instill proper safety precautions by requiring everyone to wear a mask at all times while indoors. (Which is what most responsible business offices and landlords of business buildings are doing.) They also did not consider the role AC unit fan systems play in spreading viral particles within a building. Not requiring everyone to wear a mask whenever they are indoors is forcing all others who might have a medical condition or worried about catching the virus to be exposed to all of the air droplets coming out of the mouths of people who refuse or choose not to wear a mask. This person was very uncomfortable with the requirements of the office but needed her job and so she wore a mask in the building every day and one of her coworkers even ridiculed and laughed at her for wearing the mask. In less than two weeks time someone reported that they had tested positive and everyone was allowed to go back to work at home again for a short period of time until they could regroup.
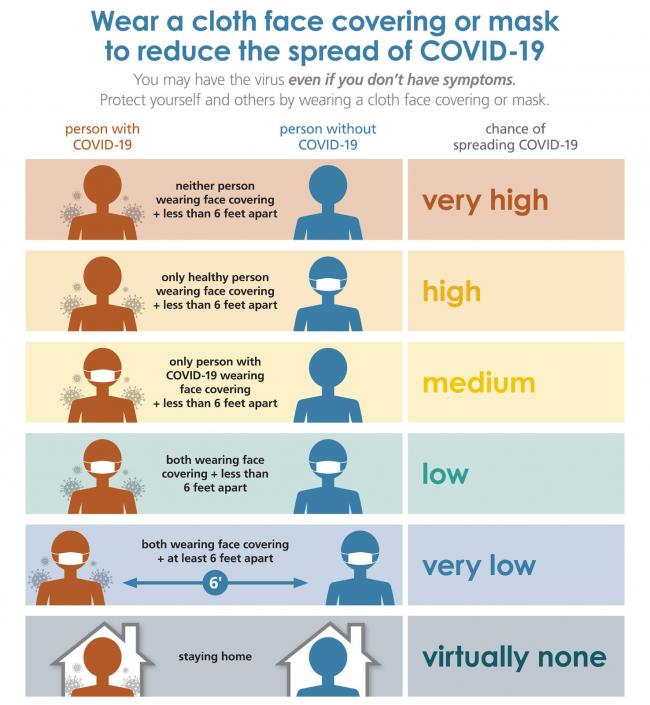
The point of sharing this story above is to encourage everyone to stop for a moment and think about who they are exposed to and who they might be exposing. None of us could possibly guess the medical conditions that people might have that we walk past in a grocery store, or a restaurant, or any other public place. The person that you’re walking by might have a child at home with sickle cell anemia, or a family member going through chemotherapy for cancer, or they themselves may have an autoimmune disorder of which you could not possibly be aware. While wearing a mask does decrease your risk of getting the virus by five times, it also decreases your risk of unintentionally sharing infected particles that could be coming from your speaking or breathing in the vicinity.
Virus Are Unique in Survivability
Rhinovirus (common cold) lives on surfaces less than an hour
Noroviruses (GI) can survive for weeks on surfaces
HIV can only live outside the body for 9-11 seconds
Hepatitis B can live on surfaces for over 60 days
How long COVID-19 can live on surfaces is not fully understood so cleaning regularly around anyone infected or suspected to be infected is important.
Your Body’s Defenses
Antibody, also called immunoglobulin, is a protective protein produced by the immune system by B cells (lymphocytes, a type of white blood cell) in response to the presence of a foreign substance, called an antigen.
During the last 3 months of pregnancy, antibodies from the mother are passed to her unborn baby through the placenta (passive immunity) – Antibodies are also passed through breast milk. After this start in life boost, other antibodies are made through either obtaining vaccines to create them or by contracting an illness and fighting the illness off.
Antibodies recognize and latch onto antigens in order to remove them from the body. Antigens can include disease-causing organisms and toxic materials such as insect venom.
B-cells fight bacteria and viruses by making Y-shaped proteins called antibodies, which are specific to each pathogen and lock onto the surface of an invading cell and mark it for destruction by other immune cells.
There are two main types of T-cells: helper T-cells and killer T-cells. Helper T-cells stimulate B-cells to make antibodies and help killer cells develop. Killer T-cells directly kill cells that have already been infected by a foreign invader. T-cells also use cytokines as messenger molecules to send chemical instructions to the rest of the immune system to ramp up its response.
Cytokines are small proteins that coordinate a response against infection and trigger inflammation. Sometimes the body can go into overdrive and cause unintentional consequences.
COVID-19 enters the body and triggers an immune response calling immune cells to the region to attack the virus. It results in inflammation and that inflammation then activates more immune cells in a vicious cycle that can harm or kill the person the immune system is trying to protect. This is called a Cytokine Storm.
Cytokine storms are a common complication of many respiratory diseases like coronaviruses, SARS, MERS, and non-infectious diseases like multiple sclerosis, pancreatitis, and rheumatoid arthritis.
With most coronavirus strains, once infected and then recovered, the remaining antibodies have given immunity to patients to the specific virus for months or sometimes years, but COVID-19 carries a big question mark.
There have been reports of patients who seem to have recovered, but then tested positive again. Some scientists believe that these cases might represent cases where there was lingering infection as opposed to reinfection, but we still have more to learn.
Antibodies are normally produced in the body around 7-10 days after the initial onset of a virus. A positive test after recovery might also be detecting residual viral RNA after the actual virus has stopped.
We still do not yet know for sure how long one remains immune (if at all) to a reinfection of COVID-19.
Herd Immunity Isn’t an Option
Some of you may have seen many people promoting the idea of herd immunity. The idea of herd immunity is that we should allow everyone to become infected knowing that some people will not make it. This idea is a survival of the fittest concept that seems archaic and inhumane in a modern society.
One should also consider the many articles, journals, and scientific papers that have come forth over the last several months demonstrating long-term health consequences of a large percentage of people who have had this virus. Complications such as myocarditis and neurological complications are not the type of aftermath that people are accustomed to after their body fights off a virus. We also do not know what long-term consequences the virus might have on the human body and it will be some time before we have enough information to better understand its behavior and its overall effect on our systems.
Closing Thoughts
I have seen social media sites aflutter with the left upset with those on the right for not wearing masks or calling it a hoax (when it clearly is a very real problem) and those on the right upset blaming the protestors (although I saw most of them wearing masks and distancing). We must work to stop this infighting and come together.
At this point, does it really matter who started the fire? We clearly have a massive fire to put out. We can sort the rest out later.
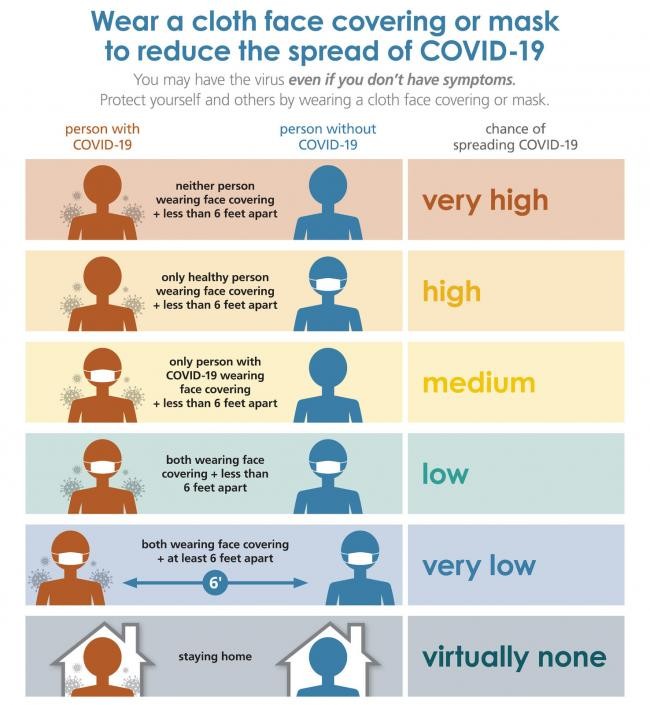
I implore you to please take this pandemic seriously and wear masks at all times whenever you are indoors or in enclosed spaces and even consider them when you are in crowds outside and cannot distance. The picture below encourages at least a cloth covering (this was because we had a huge shortage of N95 masks (which are ideal) that are in greater demand for healthcare providers and responders. An N95 is the best mask for protection overall.
Brian holds a Master degree in Health Administration (MHA), a Bachelor of Science in Health Sciences (BSHS), and a Certificate in Clinical Bioethics which bestows the ability to serve on ethics boards, help make healthcare decisions, and provide continuing medical education.
He is a national author and speaker and health consultant in all aspects of healthcare delivery, with special interests in risk adjustment, population health, public health, clinical bioethics, patient safety, and patient education.
*All posts and materials posted here are for education and demonstration purposes and are not intended to be medical advice. It is important to remember that every person is unique with unique diagnoses, and may be taking different prescriptions and supplements. I encourage each person to discuss your conditions with a trusted healthcare provider and be engaged to learn along your individual path to wellness.
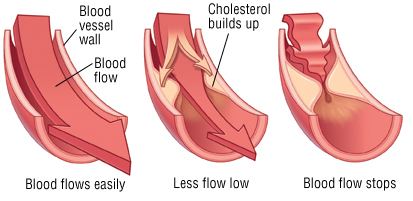
Hypercholesterolemia is the diagnosis of having elevated levels of cholesterol in the blood. It is a type of hyperlipidemia (high levels of lipids in the blood). Cholesterol is measured through blood analysis, and can be affected by diet so much that a fasting blood sample is necessary to gain accurate results. Cholesterol is a naturally occurring substance in the body that is necessary for cell growth. It is when patients have too much cholesterol or problems with cholesterol regulation in the body that high levels can become problematic. While the word lipid is often considered a synonym for fats, fats are actually a type of lipid called triglycerides. The body needs cholesterol, fats, lipids and triglycerides, however when there is an overabundance or improper regulation occurs, patients may experience problems.
Lipid disorders, also called dyslipidemias, are abnormalities of lipoprotein metabolism and include elevations of total cholesterol, Low Density Lipoprotein (LDL) cholesterol, or triglycerides; or deficiencies of HDL (High Density Lipoprotein) cholesterol. These disorders can be acquired or familial (for example, familial hypercholesterolemia). Total cholesterol is a generic overall value, while HDL is a healthy form of cholesterol and LDL is a bad form of cholesterol. LDL can further be analyzed for variations in fluffy sticky cholesterol cells as opposed to smaller and less serious cells. To remember the difference between HDL and LDL, just remember that “H” stands for healthy.
Cholesterol can create blockages of normal blood flow (Atherosclerosis)
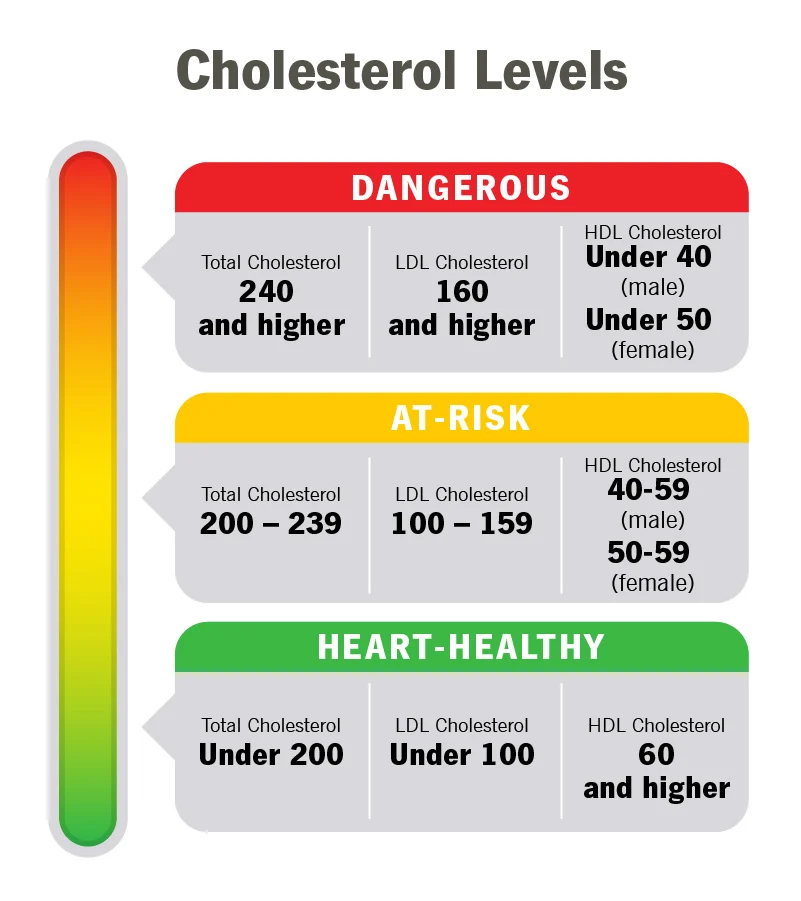
Understanding Lab Values:
Total blood cholesterol: This includes your HDL, LDL, and 20 percent of your total triglycerides.
Triglycerides: This number should be below 150 mg/dL. Triglycerides are a common type of fat. If your triglycerides are high and your LDL is also high or your HDL is low, you’re at risk of developing atherosclerosis.
HDL: The higher this number, the better. It should be at least higher than 55 mg/dL for females and 45 mg/dL for males. HDL is “good cholesterol.”
LDL: The lower this number, the better. It should be no more than 130 mg/dL if you don’t have heart disease, blood vessel disease, or diabetes. It should be no more than 100 mg/dL if you have any of those conditions or high total cholesterol.
Chart courtesy of Cleveland Clinic, link below
What you can do:
Decrease fat intake: The total fat in your diet should be cut back to no more than 30% of your daily caloric intake. For instance, if you consume 1,800 calories per day, you should get no more than 600 calories from fat. Reduce fatty foods such as meats, dairy (dairy milk & cheeses), egg yolks, and oils like coconut and palm. You can substitute for lower fat options like using cooking oil sprays, margarine, or canola oil. Avoid trans fats. Learn more about Trans Fats here: https://www.heart.org/en/healthy-living/healthy-eating/eat-smart/fats/trans-fat
Reduce meat intake: Pork, lamb, and beef are higher in fat than chicken and fish. Choosing leaner cuts such as eye of round and pork tenderloin can help too. Trim fatty portions from meats if you are cooking at home. Choose smaller portions- 3 ounces of meat is plenty. You can choose other foods like beans, and vegetables and protein substitutes.
Increase fiber intake: Fiber can reduce risk of heart disease. Foods high in fiber include nuts, seeds, legumes (peas, lentils, edamame, black beans, and kidney beans), whole grains (barley, oats – oatmeal is a great addition to a cholesterol lowering diet- whole wheat breads and whole wheat pastas), vegetables, and fruits (especially blackberries, grapefruits, apples, bananas, pears, and oranges).
Lower alcohol intake: Too much alcohol can boost triglycerides. Excess alcohol is linked to obesity and weight gain. “Moderate alcohol use” means no more than 2 drinks per day for men and no more than 1 drink per day for women. Avoiding alcohol altogether is even better.
Exercise regularly: A minimum of 2.5 hours of exercise per week is recommended to include running, swimming, walking, weight lifting, yoga, and hiking. Slowly increase your time by starting out with 10-15 minutes and gradually increase your time to ease into a more regular schedule.
Brian holds a Master degree in Health Administration (MHA), a Bachelor of Science in Health Sciences (BSHS), and a Certificate in Clinical Bioethics which bestows the ability to serve on ethics boards, help make healthcare decisions, and provide continuing medical education.
He is a national author and speaker and health consultant in all aspects of healthcare delivery, with special interests in risk adjustment, population health, public health, clinical bioethics, patient safety, and patient education.
*All posts and materials posted here are for education and demonstration purposes and are not intended to be medical advice. It is important to remember that every person is unique with unique diagnoses, and may be taking different prescriptions and supplements. I encourage each person to discuss your conditions with a trusted healthcare provider and be engaged to learn along your individual path to wellness.
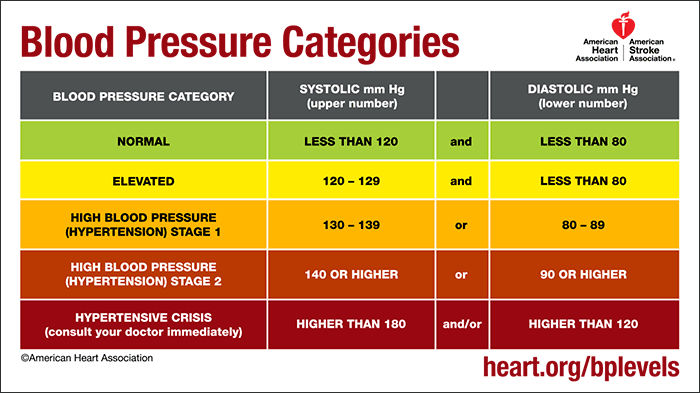
Hypertension is a chronic medical condition where the blood pressure in the arteries is elevated above normal ranges. There are two portions of a blood pressure reading: the top number represents the systolic number (the heart is contracting, systole), and the bottom number represents the diastolic number (the heart is relaxed between beats, diastole). Normal ranges for an adult reading is in the range of 100-140mmHG systolic and 60-90mmHG diastolic. High blood pressure is often diagnosed when readings exceed 140/90 over multiple measurements over time.
Hypertension is a diagnosis where a patient has a chronic elevated blood pressure of the arteries, which makes the heart muscle work harder than normal. While blood pressure changes with activity, mood, etc., it is measured by when the heart is contracting (systole) or relaxing between beats (diastolic). While there are various normal accepted blood pressures, and even variable norms for different patients that can change based on age, racial group, and size of patient. It is also generally accepted that high blood pressure is present when a patient continually has a reading of 140/90 mmHg or above. Hypertension can be primary meaning that it is not due to other diagnosis, or secondary meaning that it is a result of some other related diagnosis.
Symptoms of High Blood Pressure:
Severe headache.
Fatigue or confusion.
Vision problems.
Chest pain.
Difficulty breathing.
Irregular heartbeat.
Blood in the urine.
Pounding in your chest, neck, or ears.
Untreated High Blood Pressure: Hypertension as a diagnosis is serious. Hypertension can lead to other complications such as vision problems, stroke, heart attack (MI), heart failure, peripheral arterial disease (PAD) and is very often the major cause of CKD (chronic kidney disease) and kidney failure.
Brian holds a Master degree in Health Administration (MHA), a Bachelor of Science in Health Sciences (BSHS), and a Certificate in Clinical Bioethics which bestows the ability to serve on ethics boards, help make healthcare decisions, and provide continuing medical education.
He is a national author and speaker and health consultant in all aspects of healthcare delivery, with special interests in risk adjustment, population health, public health, clinical bioethics, patient safety, and patient education.
*All posts and materials posted here are for education and demonstration purposes and are not intended to be medical advice. It is important to remember that every person is unique with unique diagnoses, and may be taking different prescriptions and supplements. I encourage each person to discuss your conditions with a trusted healthcare provider and be engaged to learn along your individual path to wellness.
Diabetes is a condition where there is
too much sugar in the body for long periods of time. There are strong genetic
factors related to some forms of diabetes, while other forms are attributed to
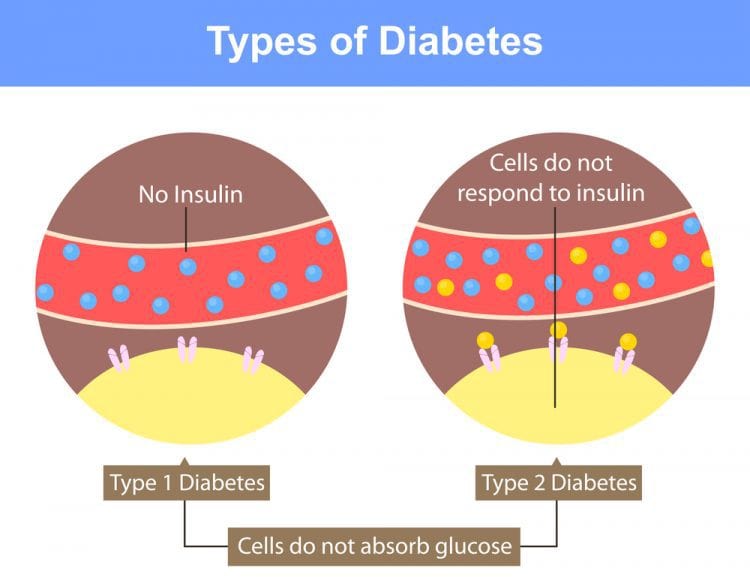
weight gain and lack of exercise. The pancreas makes insulin, which helps the
body use consumed sugars. Diabetes is
caused by either the pancreas not producing enough insulin, or the cells of the
body are unable to respond to the insulin produced. There are 4 main types of diabetes:
Type 1 = the body’s failure to produce enough insulin. This was previously known as “insulin-dependent” diabetes mellitus (IDDM), or “juvenile diabetes.”
Type 2 = this starts with “insulin resistance,” where the cells fail to use the insulin produced properly, but can progress to a lack of insulin over time. This was previously known as “non-insulin-dependent” diabetes mellitus (NIDDM), or “adult onset” diabetes.
Gestational Diabetes = when pregnant women without a previous history of diabetes develop high blood sugars during pregnancy requiring close monitoring. Many of these patients may convert back without diabetes after delivery, while others may continue to have diabetes.
Secondary Diabetes = when a patient without previous history of diabetes develops high blood sugars, usually as a result of: (a) an underlying condition, such as Cushing’s syndrome or pancreatitis, (b) a drug or chemical, such as steroidal use, or (c) a surgical procedure, such as a pancreatectomy. A wide range of health problems that damage, injure, interfere with, or destroy the pancreas can cause secondary diabetes. If the underlying cause of secondary diabetes can be successfully treated, insulin production may improve or return to normal. Common causes include:
Chronic pancreatitis occurs when digestive enzymes attack and destroy the pancreas. The main causes of chronic pancreatitis are alcoholism, blocked or narrow pancreatic duct due to some form of trauma or cyst, and heredity.
Cushing’s disease is a hormonal disorder caused by prolonged exposure of the body’s tissues to high levels of the hormone cortisol spontaneously produced by the adrenals, or by excessive use of cortisol or other similar steroid hormones (i.e., steroids used to treat life threatening diseases such as asthma, rheumatoid arthritis, systemic lupus, inflammatory bowel disease, chronic allergies, etc.).
Cystic fibrosis is a genetic disease that causes the incapacitation of the pancreas by fibrosis and can lead to the development of Type 2 Diabetes.
Adenocarcinomas are cancers that begin in cells that line the inside of organs. Almost all pancreatic cancers are of this type.
Drugs (chemically induced diabetes).
Type 1 vs. Type 2
The importance of insulin is that it enables the body to use consumed sugars as energy. In fact, most diabetic complications arise from the inability to use these sugars. When left roaming in various areas of the body, the excess unused sugars can cause very serious complications. In type two diabetes, which tends to be more common than type one, the patient either does not make enough insulin or is unable to use the insulin the body makes for various reasons. These patients may be placed on an oral medication, an insulin supplement, or a combination to help regulate blood sugar levels.
There are some ethnic groups who are at a higher risk for developing diabetes, which include American Indians, African Americans, Latinos, Asian Americans, and Pacific Islanders. An important factor in controlling diabetes is through diet and exercise. However, even the best-intention patient may find difficulty navigating the ingredient labels of some foods as sugars can come in a variety of types which may be unnoticed by the novice patient. Economically, it is also more difficult for diabetics as their health food lifestyle is typically much more expensive.
While diabetics often check their blood sugars between one to four times a day, the ultimate blood sugar test is the hemoglobin A1C, which is often referred to as A1C. While regular blood sugar readings report current blood sugar levels, the A1C gives a blood sugar average for the past three months. This test is the gold standard used by physicians to monitor the control of the diabetic’s blood sugar. Typically, anyone with an A1C of seven or less is considered to be controlled and those who are over seven will often have changes made to the medications or insulin dosing or both.
Low vs. High Blood Sugar Readings : Slight fluctuations in blood sugar levels are completely normal and also happen on a daily basis in people who do not have diabetes. Between around 60 and 140 milligrams of sugar per deciliter of blood (mg/dL) is considered to be healthy. This is equivalent to blood sugar concentrations between 3.3 and 7.8 mmol/L. “Millimole per liter” (mmol/L) is the international unit for measuring blood sugar. It indicates the concentration of a certain substance per liter.
Checking Blood Sugar Levels : People with type 2 diabetes should take a blood sugar reading at least once a day. Some may need to test as frequently as seven times a day. Doctors recommend that people who need insulin to treat their type 2 diabetes perform three or more blood sugar tests throughout the day, especially if they take multiple daily doses or are using an insulin pump. Most people use a small glucometer machine to check their blood sugars regularly, and it is important to track these readings so that your healthcare providers can get a better idea of how your body is responding to your daily activities to include foods. It is important to keep a food diary, along with a record of what you were doing throughout the day (sitting long periods vs. working out or running, etc.) so that a treatment plan can better be customized to your situation. There are many phone apps that provide easy to use trackers for tracking foods eaten, activity levels and blood sugar readings.
Blood Tests Used
Random blood sugar test. Blood sugar values are expressed in milligrams per deciliter (mg/dL) or millimoles per liter (mmol/L). Regardless of when you last ate, a blood sample showing that your blood sugar level is 200 mg/dL (11.1 mmol/L) or higher suggests diabetes, especially if you also have signs and symptoms of diabetes, such as frequent urination and extreme thirst.
Fasting blood sugar test. A blood sample is taken after an overnight fast. A reading of less than 100 mg/dL (5.6 mmol/L) is normal. A level from 100 to 125 mg/dL (5.6 to 6.9 mmol/L) is considered prediabetes.If your fasting blood sugar is 126 mg/dL (7 mmol/L) or higher on two separate tests, you have diabetes.
Oral glucose tolerance test. This test is less commonly used than the others, except during pregnancy. You’ll need to fast overnight and then drink a sugary liquid at the doctor’s office. Blood sugar levels are tested periodically for the next two hours.A blood sugar level less than 140 mg/dL (7.8 mmol/L) is normal. A reading between 140 and 199 mg/dL (7.8 mmol/L and 11.0 mmol/L) indicates prediabetes. A reading of 200 mg/dL (11.1 mmol/L) or higher after two hours suggests diabetes.
Glycated hemoglobin (A1C) test. This blood test indicates your average blood sugar level for the past two to three months. Normal levels are below 5.7 percent, and a result between 5.7 and 6.4 percent is considered prediabetes. An A1C level of 6.5 percent or higher on two separate tests means you have diabetes.
A1C levels need to be checked between two and four times a year. Discuss your target A1C goal with your doctor, as it may vary depending on your age and other factors. For most people, the American Diabetes Association recommends an A1C level below 7 percent.
An elevated A1C level may signal the need for a change in your medication, meal plan or activity level.
In addition to the A1C test, it is important to also monitor your blood pressure and take blood and urine samples periodically to check your cholesterol levels, thyroid function, liver function and kidney function. Regular eye and foot exams also are important.
Symptoms of Hyperglycemia: (High Blood Sugar)
Signs of very high blood sugar levels may include the following:
Extreme thirst, drinking a lot and then urinating frequently as a result
Unintentionally losing a lot of weight within a few weeks
Noticeable loss of energy with muscle weakness, tiredness and generally feeling quite unwell
Nausea and stomach ache
Trouble seeing
Poor concentration
Frequent infections (cystitis, thrush)
Confusion and drowsiness, or even coma
Symptoms of Hypoglycemia: (Low Blood Sugar)
Signs that your blood sugar is too low may include:
Racing pulse
Cold sweats
Pale face
Headache
Feeling incredibly hungry
Shivering, feeling weak in the knees
Feeling restless, nervous or anxious
Difficulty concentrating, confusion
Diabetes affects many other health conditions and can make a patient more susceptible to getting other new health problems to include most commonly: Neuropathy (damage to the nerves in the extremities), Retinopathy (damage to the retina of the eyes), Chronic Kidney Disease (CKD) (damage to the kidneys), Heart Disease (0ver time sugars can harm blood vessels and arteries), and Erectile Dysfunction (ED) in men (damage to the nerves and vessels supplying blood to the penis).
Brian holds a Master degree in Health Administration (MHA), a Bachelor of Science in Health Sciences (BSHS), and a Certificate in Clinical Bioethics which bestows the ability to serve on ethics boards, help make healthcare decisions, and provide continuing medical education.
He is a national author and speaker and health consultant in all aspects of healthcare delivery, with special interests in risk adjustment, population health, public health, clinical bioethics, patient safety, and patient education.
*All posts and materials posted here are for education and demonstration purposes and are not intended to be medical advice. It is important to remember that every person is unique with unique diagnoses, and may be taking different prescriptions and supplements. I encourage each person to discuss your conditions with a trusted healthcare provider and be engaged to learn along your individual path to wellness.
Welcome to Brian’s Health Blog. This is a new healthcare site that intends to provide trusted insight and educational material about the healthcare world. While opinions might also be presented on this page, they are solidified in research and education looking at all possible outcomes and potential variations. I plan to also provide some useful reference materials for various common medical conditions, medications, herbals, procedures, and interesting healthcare topics. I have a strong clinical background that started over 30 years ago in Aeromedical Evacuation in the USAF and have worked in every aspect of healthcare from the bedside to the boardroom. I hope these posts might provide enlightenment and provoke thought around refining healthcare delivery while engaging people to become proactive stewards of their own health.
Please keep in mind that none of this information or commentary is to be considered medical advice. Every person and situation is unique and you should reach out to a trusted licensed healthcare provider in your area if you are having any medical problems or concerns. Remedies, or suggestions of common treatments are also purely for educational and illustrative purposes and are not to be considered medical advice or recommendations.
Brian holds a Master degree in Health Administration (MHA), a Bachelor of Science in Health Sciences (BSHS), and a Certificate in Clinical Bioethics which bestows the ability to serve on ethics boards, help make healthcare decisions, and provide continuing medical education.
He is a national author and speaker and health consultant in all aspects of healthcare delivery, with special interests in risk adjustment, population health, public health, clinical bioethics, patient safety, and patient education.
*All posts and materials posted here are for education and demonstration purposes and are not intended to be medical advice. It is important to remember that every person is unique with unique diagnoses, and may be taking different prescriptions and supplements. I encourage each person to discuss your conditions with a trusted healthcare provider and be engaged to learn along your individual path to wellness.





{kind=link}